As of 24/10, as the country is gearing towards another ‘Emergency’ — all in the name of “combating the urgency and resurgence of Covid 19” — it might be high time to revisit what we know about Covid 19. We have been fighting this virus for a year, we now know a lot more than when we did in March, at the time of entering the first Movement Control Order (MCO). Reviewing these facts will help us dealing with the pandemics better, and avoid mass hysteria and senseless panic. While we must not underestimate the potency of the virus, we must not give in too much to the fear of it, so much so that it robs us of our joy and sense of peace, disrupts our routine, curtails our freedom and gives a pretext for a dictator to rise.
I write it as a scientifically curious reader who has no formal training in medicine and epidemiology. But you honestly don’t need a brain of Einstein and a degree in relevant fields to understand facts and statistics and to draw simple logical inferences ( unlike Quantum Mechanics and superstring theories which do require a certain level of mental sophistication to grasp) . You can independently check the facts I outline here, and check the logical inferences yourself. If my advice seems to contradict what you know or what the government tells you, you can use your brain to find out who is right. There is no need to blindly accept the arguments from authorities, and I’m not at all too sure that the “authorities” don’t have ulterior motives that that push for agendas beyond just fighting Covid and reviving economy.
A) The difference between Case Fatality Rate and Infection Fatality Rate
Before we start of, we have to understand the difference between Case Fatality Rate ( CFR) and Infection Fatality Rate ( IFR).
- CFR: the proportion of deaths compared to the total number of people diagnosed.
- IFR: the proportion of deaths compared to the total number of people actually infected
Obviously, there are people who are infected but who choose not to seek treatment because the disease is asymptomatic ( no symptom) or because of other reasons, thus the IFR will always be less than CFR. There is no precise way of knowing the actual asymptomatic carriers, although we can still estimate. Current estimates by WHO suggest that 80% of the infections are mild or asymptomatic.
The death rate that we see on newspapers, the one that our DG reported on daily basis, refers to the CFR and not IFR. Thus the CFR for our country currently stands at 0.9% as of 23/10/2020 ( 214 deaths out of 24514 cases).
B) The Case Fatality Rate is dropping in most countries
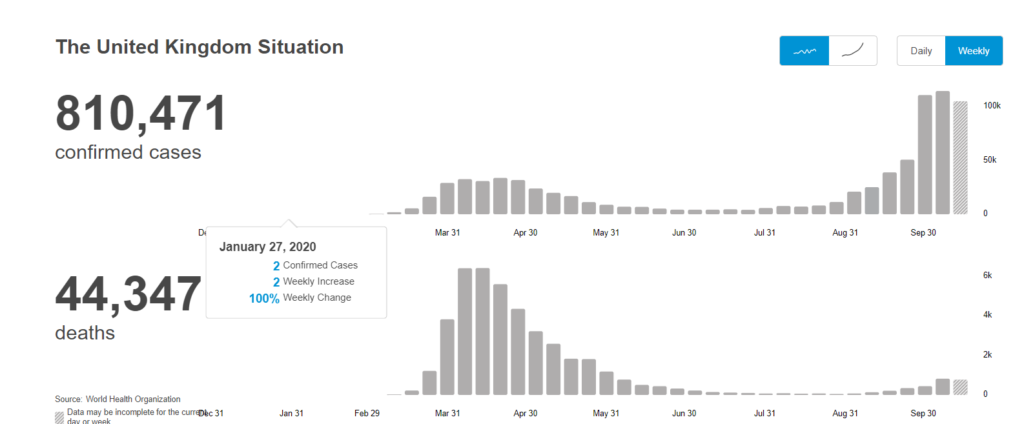
European countries are being hit hard by the second wave of Covid 19 entering September. Take UK for example, it recorded 26,000 confirmed case in a single day on 22/10/2020, 5 times as high as the highest single day record during the first wave in April.
But, what is important to note is that the death rate is a lot lower, resulting in comparatively low CFR. The highest death per day in April was around 1100 ( ~20%), but entering September/ October, the highest day on a single day is only 224 (~0.86%).
We can also observe the same trend in Malaysia.
What can explain the falling CFR? It could probably be due to any of the following factors:
- Better drugs and better care
- The virus losing its potency through some unknown mechanism
- The first wave inflicted mostly aging population while the second wave inflicts mostly young people
- More aggressive testing now compared to then.
But whatever it is, it should give us comfort that we are doing things alright. Covid 19 situation is improving, despite the appearance of high number of daily confirmed cases.
C) The Infection Fatality Rate is low, especially for younger population
A meta study by WHO reveals that the IFR ranged from 0.0% to 0.67% ( median 0.10%). Another study shows that
The estimated age-specific IFRs are very low for children and younger adults but increase progressively to 0.4% at age 55, 1.3% at age 65, 4.2% at age 75, and 14% at age 85.
For comparison sake, the IFR for seasonal influenza is below 0.1% , though we don’t really know the age breakdown of it. SARS fatality rate is 11%.
Putting these facts together, it seems that Covid 19 is only a few times more deadly than seasonal influenza at most ( this figure can be revised downwards as the population develops immunity and the true extent of asymptomatic cases is being discovered), but an order of magnitude or so less deadly than SARS. Is the initial fear surrounding Covid 19 well-founded? Or is it just a mass hysteria? I am now inclining to think it’s the later, somehow we blew the fear out of proportion.
Also, this would suggest that one needs to protect the parents more than the children, as the children as a group is suffering the lowest mortality rate. In the light of this, it simply makes no sense to close the childcare but not office; leaving the issue of who will take care of kids at home, aren’t adults are more susceptible and hence require more protection than children?
So should I be scared? Read more here.
D) What about Excess Death?
Different countries might have different ways of ascertaining the cause of a death, and not all Covid 19 inflicted patient died in the hospital, some might die at home, with the cause of death attributed to something else. So the official death count almost always undercounts.
But, on the other hand, the true number of infections is always higher than the recorded number of infections, so the CFR, although can be calculated precisely, always exaggerates the actual deadliness of a virus. Two factors tend to cancel each other out, epidemiologists often turn to the Excess Death, the extra deaths that happen compared to the expected death to gauge the true impact of a virus.
Here are the four countries’ recorded death for the year 2020:
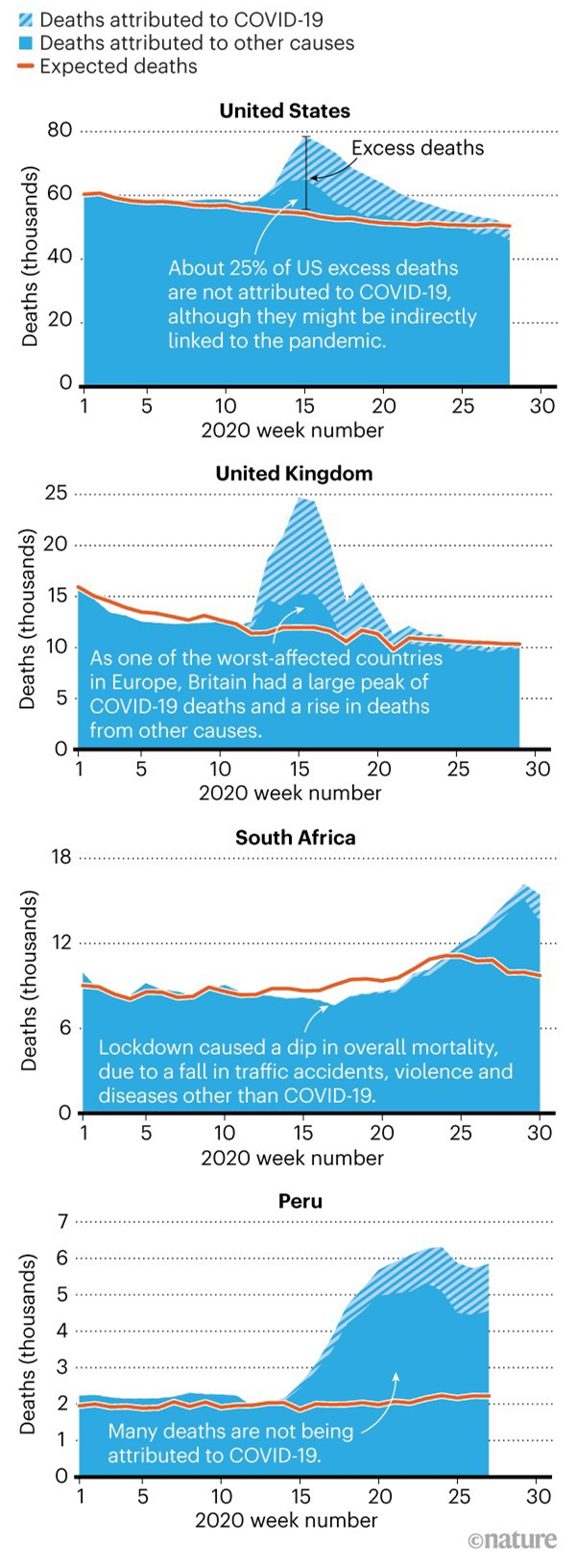
A few observations:
- Despite no more lockdown in Autumn and after, and despite a hike in diagnosed case, the Excess Death in US is gradually going back to normal line.
- While UK is currently tightening the lockdown rules, it is important to observe that the excess death is going back to normal, even when the effects of second wave sinks in.
- But the Excess Death in Peru and South Africa is picking up steam.
- But also, as noted in the Nature article, in the reversal of the above point, there are some countries, such as Bulgaria, have even experienced negative excess deaths.
- Although the excess death must have something to do with Covid 19, but it’s unclear whether it’s due to the patients succumbing to the virus, or because of bad policies that were designed to stop Covid in the first place. The graphs didn’t break them out. It is entirely possible that doing nothing will end up with less excess death that enacting bad policies. I’m not saying that this must be the case, but just that the graphs above don’t tell us enough.
As the Nature article says, we still don’t quite know how to interpret this data, but it may suggest that just like past pandemics, the Covid 19 will only succeed in killing in those who are most vulnerable, and its potencies will decline over time.
E) Movement Control Order (MCO) or Lockdown is meant to “flatten the curve”, nothing more
One big misconception about MCO is that we can win the battle against Covid 19 by forcing everyone to stay at home. Well, no. The most we can do by staying at home, is to reduce the spread of the virus, so that we don’t overwhelmed the medical resources that we have. This is the true meaning of flatten the curve, not to defeat the virus. You can’t defeat the virus because the moment you start going out and going to work, the virus will come back with a vengeance.
To put it more crudely and perhaps a little bit less accurately, those who are going to die from Covid 19, are still going to die anyway. But MCO will make them die later rather than now, the benefits of this is multifold:
- The potential Covid patients get to enjoy more months of lives
- They won’t overwhelmed our medical resources, and prevent other needy from using it.
Until a vaccine is found, or when herd immunity is reached, there is no way to defeat the virus. We will talk more about this later.
F) Lockdown also kills people, but are we measuring it?
One argument advocating total lockdown against all other alternatives, is that human lives are invaluable. We need to shut down our economy to save lives! We can always earn money later but we can’t resurrect our love ones! A WhatsApp message gone viral put this school of thought perfectly:
And yes, who can argue against preserving lives? But of course, truth is always more complicated than simple slogans.
The fact is that, lockdown also kills people, either the restrictions cause significant unintended consequences such as lack of access to critical healthcare, or a spike in suicides due to excessive boredom locked at home, or just plain starvation due to inability to find work and food. For the last, I can imagine that the people in the slums would prefer to just get to work and suffer the risks of being infected by Covid 19, rather than being forced to stay at home and suffer starvation. After all, a study in India finds that IFR is only 0.05% to 0.10% in slums, despite that the sanitary conditions are generally poor and they are usually lack of healthcare support.
G) Can we count on vaccine?
Russia tells us that their vaccine “Sputnik V” is now available for consumption. China also tells us that their vaccine is now ready for mass testing and exports. So is our plight nearing the end?
It is important to remember that Russia and China were rushing the vaccines not because they were far ahead in terms of Covid research ( far from it!), but because they wanted to score political points. Their vaccines have not undergone proper, vigorous and stage 3 testing as it is required by normal standards. In other words, use them at your own risk!
Why do vaccines take a long time to develop? Finding the right vaccines is effectively an exercise to find a needle in the haystack. Our past experience in developing SARS vaccine can help, but we still need enough time to see whether the vaccines work as intended and without side effects. Finding a vaccine has more to do with luck than technology.
And then there is this problem of virus mutation, which threatens to render a vaccine completely ineffective. Virus mutates all the time, most of the mutations are harmful, but some can be beneficial ( to the virus, not to us), which increases its deadliness against human. What happens if a Covid 19 successor–let’s called it Covid 20– comes along? No one knows whether the vaccines developed for Covid 19 are still usable. In the worst case scenario we just have to start over.
If history is any guide, we shouldn’t be too sanguine. Spanish flue devastated the world in the early 20th century, and we didn’t vaccinated it out of existence; we just developed herd immunity( those who didn’t, just died). Likewise, we didn’t develop an effective vaccine against SARS; it died because it was so deadly and thus made it easy to contain. In the end, we isolated SARS out of existence.
For seasonal influenza, we still don’t have a generic vaccine against it, because it always mutates and it’s not easy to take the human carriers out of the population, precisely because it has no symptom on the majority of the carriers.
Taken these lessons together, it implies that although Covid 19 is more deadly than influenza and hence make it more detectable, there still exists a majority portion of asymptomatic carriers that are hard to isolate, so it’s unrealistic to hope that we can isolate Covid 19 out of existence like how we did it for SARS. And given that we still don’t have effective generic vaccine against influenza for so long, it’s not realistic to hope that we can have one against Covid 19 in a short order of time, say 3~5 years.
[Update 24/11/2020: Now we have not just one but three promising Covid 19 vaccine. Future looks good. However we might still have to wait until next year June before life returns to all its normalcy]
So, is our government doing a good job?
This is a political question, not really an epidemiology one.
A lot of people “feel” that the government is doing a FABULOUS job because
- Our mortality rate and infection rate are low compared to other neighboring countries like Indonesia and Philippines.
- They get the enjoy “work from home” with full pay and benefits.
Their feeling is not based on any scientific or even rational thinking ( a reminder that democracy may not be good if the underlying people can’t think). It’s important to remember that the real tests for Covid 19 don’t come during the time when the first wave of the pandemic rages; the real tests come when one has to coexist with it.
Essentially I suppose that there is a graph for mortality rate vs. economy growth, with a monotonously increasing relationship between the two variables. The government has to pick the right point to manage, and make sure that there is no excess mortality rate other than absolutely necessary, and/or the economy growth is not truncated other than necessary. In other words, the government is doing a good job only when it succeeds at protecting its people and also keeping the economy running.
So far our government seems to be managing for a point located at the spectrum of lower mortality rate and economic growth, but whether this is the best for the country, we will still have to see.
Is our government doing a good job? As far as election is concerned this question may not be so important; what is important is how well the politicians can manage ( read: manipulate) the people’s perception. Which is why I said: this is a political, not an epidemiology question.
Should I be scared?
If you are young and healthy, no, you really shouldn’t be scared. Let’s put the number in perspective: the US has a mortality rate from car accidents per capita of 0.01%/year, and the CDC’s best guess infection fatality rate estimate for the 20-49 age group is 0.02%/infection. Keep in mind that the 0.02%/ infection already includes adults who have medical conditions. A healthy adult’s mortality rate will be far lower than this.
Ask yourself this question, young man and woman, will you stop driving if the road is twice as dangerous as now? Will you be scared? If no, then why should you be scared of Covid?
Of course if you have prior medical conditions, and you are above age 50, then the risks go up dramatically ( For the 50-69 age group, the CDC estimates a 0.5% IFR, so COVID-19 would be 25x higher mortality than random car crashes).
Instead of a blanket lockdown, it would be ideal if the government has a way to protect the elderly and the sick, and just let the young people resume working. But so far this is not happening.